Vibrant CTD
The most comprehensive, sensitive, and specific test to assist in the diagnosis of connective tissue disorders (CTD) and related autoimmune disorders.

3.6 years
3.6 years is the average time that patients suffer symptoms before meeting diagnostic criteria1.
>2 million
>2 million Americans have rheumatoid arthritis (RA)2.
3% of people
3% of people over 50 years old have Sjögren’s syndrome3.
Prevalence of ctd in north america
Disease
Prevalence
Rheumatoid arthritis (RA)
1/116
Systemic lupus erythematosus (SLE)
1/4,200
Sjögren’s syndrome
1/6,940
Polymyositis/
dermatomyositis
1/20,000
more common in women
Disease
Women:Men
SLE
RA
Sjögren’s
SSc
MCTD
6-10:1
3:1
9:1
5-14:1
3:1
Symptoms
- Connective tissue disorder (CTD) is a group of medical diseases that has the connective tissues of the body as a primary target of pathology.
- Most CTDs feature abnormal immune system activity with inflammation in as a result of an immune system that is directed against one’s own body tissues (autoimmunity).
Symptoms and conditions associated with CTD
- Hair loss
- Muscle pain
- Numbness or tingling in the hands or feet (Raynaud’s Syndrome)
- Inflammation and damage to organs and tissues, including the kidneys, lungs, heart, lining of the heart, central nervous system, and blood vessels
- Low-grade fever
- Persistent fatigue, weakness
- Arthritis-like pain in one or more joints
- Red rash (for lupus, one resembling a butterfly across the nose and cheeks)
- Skin sensitivity to light
Early signs of CTD
- General feeling of being unwell: This might include a mild fever and increased fatigue.
- Swollen/Puffy Fingers: Swelling in the hands and fingers is a common symptom of CTD.
- Raynaud’s Phenomenon: This is experienced as cold/numb fingers, toes, tip of the nose, and ears that may change color in response to cold. This is caused by a reduction in blood flow to these areas
- Muscle and joint pain: The symptoms of rheumatoid arthritis including muscle aches and joint swelling/pain are common in CTD.
- Pulmonary hypertension (PH): This condition means that there is an increased pressure in the pulmonary arteries. These are the arteries that carry blood from your heart to your lungs to pick up oxygen. PH can cause symptoms such as shortness of breath during routine activity, fatigue, chest pain, and a racing heartbeat. As the condition gets worse, its symptoms may limit all physical activity
CTD includes but is not limited to
- Systemic Lupus Erythematosus (SLE): SLE is a widespread and chronic autoimmune condition that, for unknown reasons, causes the immune system to attack the body’s own tissues and organs, including joints, kidneys, heart, lungs, brain, blood, and skin.
- Sjogren’s Syndrome: In Sjögren’s, white blood cells attack moisture-producing glands, such as the tear ducts and salivary glands, making it difficult for your body to produce saliva and tears.
- Systemic sclerosis (also known as scleroderma): Scleroderma can cause the tightening and hardening of the skin and the connective tissues. The word “scleroderma” derives from two Greek words: “sclero” meaning hard, and “derma” meaning skin.
- Rheumatoid Arthritis (RA): RA is a chronic inflammatory condition and autoimmune disorder that generally affects the lining of the joints in your hands and feet. Rheumatoid arthritis causes a painful swelling that can eventually lead to deformity and erosion of your joints and bones.
- Polymyositis: Polymyositis (pol-e-mi-o-SI-tis) is a persistent inflammatory muscle disease that causes weakness of the skeletal muscles, which control movement.
- Dermatomyositis: Dermatomyositis (dur-muh-toe-my-uh-SY-tis) is an uncommon inflammatory disease marked by muscle weakness and a distinctive skin rash.
Early detection of CTD is important because CTD is closely associated with other diseases
- Raynaud’s Phenomenon: Raynaud’s phenomenon is a problem with blood flow. This means that your body is not able to send enough blood to your extremities, like your hands and feet, so they tend to feel very cold, numb or tingly and can even discolor due to lack of circulation.
- Neuropathy (or peripheral neuropathy): Peripheral Neuropathy, is nerve damage that often causes weakness, numbness and pain, usually in your hands and feet, but may also occur in other areas of your body, it may also signal lupus.
- Anemia: Anemia is a condition in which your blood has a lower than normal number of red blood cells causing symptoms such as weakness, fatigue, dizziness, shortness of breath, or headaches. Long-lasting or severe anemia can damage the body’s vital organs and in extreme cases, death.
- Pleurisy (also called pleuritis): Pleurisy is an inflammation of the moist, double-layered membrane that surrounds the lungs and lines the rib cage, making breathing extremely painful.
What is tested
What is tested
Vibrant CTD is a diagnostic test that offers the most comprehensive panel for the connective tissue disease (CTD) spectrum.
Vibrant ANA IFA
Homogeneous
ENA Profile-10
Rheumatoid Arthritis Associated
markers
SLE Associated marker
HOW DO YOU ORDER VIBRANT’S CONNECTIVE TISSUE DISORDER TEST?
Vibrant’s connective tissue disorder test is only available to order through your provider. If your physician is not in our network, please contact us.
why vibrant
Vibrant CTD – Simple blood test to identify, monitor and manage CTD.
- Only Vibrant America offers multiple tests in one comprehensive platform.
- Detecting well-established CTD serological biomarkers.
- Early detection may help optimize therapeutic outcomes4.
- Rule out CTD and autoimmune diseases.
- More sensitive and specific than performing one test alone.
Vibrant’s comprehensive CTD panel can fill in the gaps of CTD diagnosis
What We Offer
Vibrant America utilizes a unique microchip platform to perform the most comprehensive serologic tests for detecting well-established CTD biomarkers from a single blood draw. Taking VibrantTM CTD is a straightforward and rapid way to predict, identify, monitor, and manage CTD.
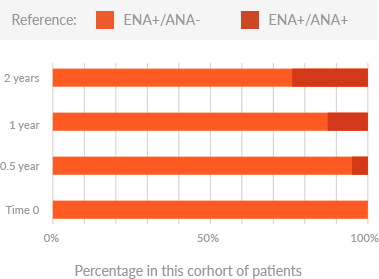
- False negatives are usually caused by testing too early before certain auto-antibodies have developed or will develop due to individual differences.
- Vibrant America conducted a 2-year follow-up study for 110 CTD-suspectedpatients and revealed that 21% of patients were ENA positive for an average of 385 (±144) days before their ANA became positive.
- A lower false negative rate can be assured by performing an all-inclusive biomarker test for CTD at Vibrant America.
- Physicians can learn about patients’ conditions at an early stage and the patients may suffer from less symptoms due to a shortened diagnostic period.
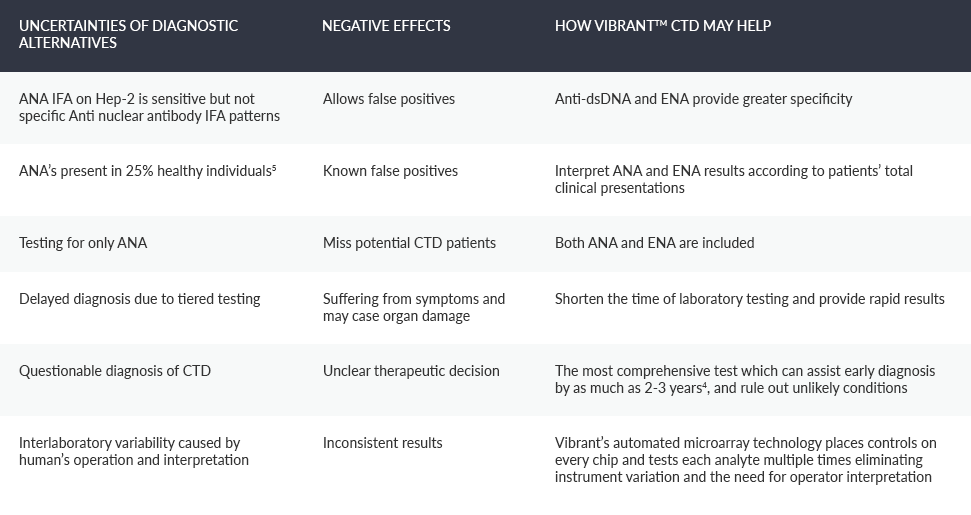
False positives may mislead a physician’s decision on diagnosis and treatment to a patient. Vibrant America can help reducing false positives from two ways:
(a)ANA testing can cause a significant number of false positives because a 1:40 dilution is usually suggested as a good dilution to screen for ANA but low-titer positive results might occur in 25% apparently healthy persons.9 Vibrant America always interpret the ANA results (1:40, 1:80, 1:160 dilutions) considering the patient’s total clinical presentation to lower the possibility of false positives;
(b) A multiplex platform of 5 tests provides serologic information to achieve a comprehensive overview of a complex condition and may help ruling out false positive.
- 50% of CTD patients are estimated to have an unclassifiable profile at disease onset.7
- Vibrant’s comprehensive CTD panel may resolve the questions and doubts for the patients who have an undefined disease.
- VibrantTM CTD is designed to provide all laboratory tests recommended by ACR and EULAR with an aim to identify conditions at an early stage.
- Upon delivery of reliable and consistent serologic reports from a laboratory with greater experience, the physician may have better clarity interpreting the results and determining an undifferentiated CTD more efficiently.
- Autoimmune disorders may take years to evolve from very subtle abnormalities to demonstrating typical features that could be recognized during an examination.
- VibrantTM CTD is a valuable tool that can detect a variety of abnormal antibodies commonly found in blood years before symptoms develop.
- This is especially true for patients with overlaping syndromes whose clinical features are usually mild.8
- Detection of the typical antibody biomarkers can assist in predicting the development of autoimmune diseases. Vibrant America provides the only diagnostic test that predicts future development of CTD and associated autoimmune diseases.
- It also provides insight when the clinical picture changes – a repeat VibrantTM CTD test can offer information regarding possible medical condition changes (to a recognizable disease, a different prognostic subgroup, or a recovery status).


- PM: Polymyositis
- DM: Dermatomyositis
- RA: Rheumatoid Arthritis
- CREST: Calcinosis, Raynaud disease, Esophageal motility disorder, Sclerodactyly, and Telangiectasia
- SLE: Systemic Lupus Erythematosus
- MCTD: Mixed Connective Tissue Disease
*The figure is developed by Vibrant America based on ACR guidelines. It is provided for information purposes only and is not intended medical advice. A physician’s test selection and interpretation, diagnosis, and patient management decisions should be based on his/her education, clinical expertise, and assessment of the patient.
This test has been developed and its performance characteristics determined by the CLIA-certified laboratory performing the test. This test has not been cleared or approved by the U.S. Food and Drug Administration (FDA). Although FDA does not currently clear or approve laboratory-developed tests in the U.S., certification of the laboratory is required under CLIA to ensure the quality and validity of the tests.
1. Ungprasert P, Crowson CS, Chowdhary VR, et al. Epidemiology of Mixed Connective Tissue Disease, 1985–2014: A Population-Based Study. Arthritis Care Res. 2016;68:1843-1848.
2. Jacobson DL, Gange SJ, Rose NR, Graham NMH. Epidemiology and estimated population burden of selected autoimmune diseases in the United States. Clin Immunol Immunopathol. 1997;84:223-243.
3. Gaubitz M. Epidemiology of connective tissue disorders. Rheumatology. 2006;45(3):33-34.
4. Soto ME, Hernández-Becerril N, Perez-Chiney AC, et al, Predictive value of antinuclear antibodies in autoimmune diseases classified by clinical criteria: Analytical study in a specialized health institute, one year follow-up. Results Immunol. 2015;5:13-22.
5. Satoh M, Chan EK, Ho LA, et al. Prevalence and Sociodemographic Correlates of Antinuclear Antibodies in the United States. Arthritis Rheumatol. 2012;64(7):2319-2327.
6. American College of Rheumatology. American College of Rheumatology position statement: methodology of testing for antinuclearantibodies. 2009;1-3.
7. Alarcón GS, Williams GV, Singer JZ, et al. Early undifferentiated connective tissue disease. I. Early clinical manifestations in a large cohort of patients with undifferentiated connective tissue diseases compared with cohorts of well established connective tissue disease. J Rheumatol. 1991;18(9):1332-1339.
8. Iaccarino L, Gatto M, Bettio S, et al. Overlap connective tissue disease syndromes, Autoimmun Rev. 2013;12(3):363-373
